
REPORT
COVID-19 Order Set Usage
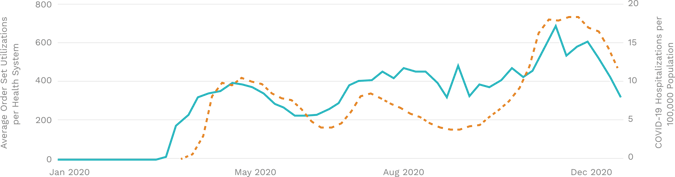
COVID-19 order set usage mostly aligned with associated hospitalizations
Although clinicians found it challenging to keep up with rapidly changing guidelines even before the pandemic, COVID-19 saw a significant proliferation of knowledge and research to help combat the disease. Health systems assisted clinicians with the development of specialized order sets to encourage best practices despite the uncertainty.
This emphasis of order set usage across health systems presents itself in an interesting way. While COVID-19 order set usage trends with national hospitalizations, it doesn’t map exactly to each successive surge. This can be seen in a lower summer hospitalization peak that corresponds with a slightly higher order set utilization peak.
As we assume these hospitalizations reflect workflows that typically require support from specialized COVID-19 order sets, it’s unclear why order set usage increases while hospitalizations decrease. This may reflect order sets being used outside of the inpatient setting as COVID-19 spread through local communities. Another hypothesis is it took time for order set adoption to diffuse throughout the health system. This uncertainty underscores the importance of linking order set usage with process or outcomes (e.g. COVID-19 hospitalizations) to truly understand how appropriately these tools are used.
COVID-19 Alert Burden
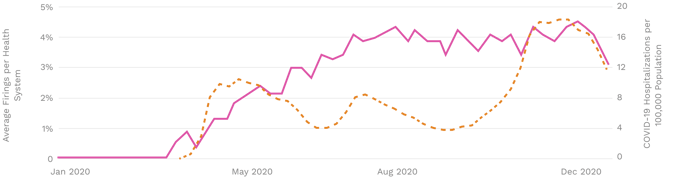
Health systems reduced the burden of interruptive COVID-19 alerts over time
Similar to order sets, custom COVID-19 alert firings weren’t directly proportional to case rates. Again, this is likely explained partly by the distinction between case rates and hospitalizations (described above). However, the sample of health systems (clients of Phrase Health) might also provide some insight. In the beginning of the pandemic, Phrase organizations might have skewed towards using more alerts than an average health system given their organizational priorities on clinical decision support.
Anecdotally, clients have suggested that the ability to do rapid process improvement cycles with Phrase’s analytics enables them to test and hone alerts rapidly. The health system partner who reported this tactic (described below), for example, was removed from this graph’s data sample because their initial alerting dramatically skewed the trend. This might suggest that new alerts and firings were added during the early periods of uncertainty and then honed as COVID-19 workflows and knowledge became established.
PCR Testing
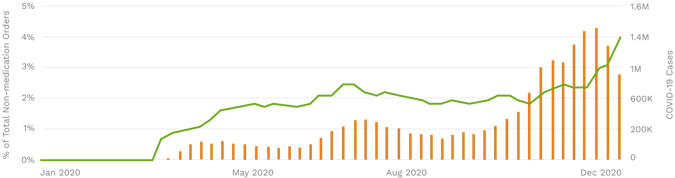
In the fall and winter, testing fell behind the rise in cases due to lack of supplies
Polymerase chain reaction (PCR) is the current gold standard for diagnosing COVID-19. Not surprisingly, testing generally followed a broader infection trend across the United States. During spikes in infections rates, one can observe a corresponding increase in testing. Interestingly, rates of PCR testing after the COVID-19 spikes in April and July don’t seem to decrease as fast as cases per week. This effect is particularly pronounced in the beginning of the pandemic when PCR tests gradually increased through July despite drops in cases. At some point in the early portion of the PCR curve, supply of PCR tests to these health systems started to catch up with demand. When the PCR tests became more broadly available, they were ordered more. However, as infection rates nearly tripled in November and December from the previous summer peak, labs around the countryreported testing shortagesof chemicals and other crucial supplies.
This might be the reason why PCR ordering peaked in this time frame, but not at a three-fold increase like the case rate. The volume of PCR tests in December--almost 5% of all non-medication orders-- not only reflects COVID-19’s burden on labs, but on workflows throughout a health system.
Hydroxychloroquine Usage
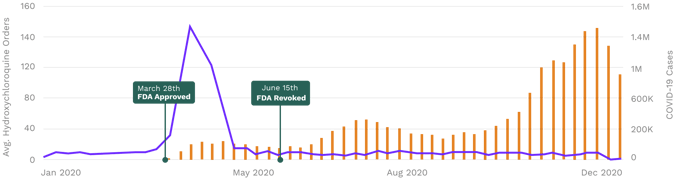
Health systems identified hydroxychloroquine was ineffective prior to FDA revocation
On March 28th, 2020, the FDA gave Emergency Use Authorization to hydroxychloroquine for treatment for COVID-19 based on early indications of effectiveness. On June 15th, less than three months later, the FDA revoked that authorization citing insufficient evidence of effectiveness and the concern it introducesdangerous cardiac riskto patients. Interestingly, hydroxychloroquine orders spiked in April and quickly reverted back to pre-COVID-19 levels almost two months prior to the FDA’s revocation. Although many had concerns about its efficacy early in the pandemic, serious doubts arose in April and May, principally when aNew England Journal of Medicine studysuggested hydroxychloroquine was not associated with a lower rate of intubation or mortality. This sudden decrease of hydroxychloroquine usage seems to show the speed at which providers and their health systems incorporate medical knowledge into practice.
Client Success Stories
COVID-19 ResourceMonitoring Through CDS
PROBLEM
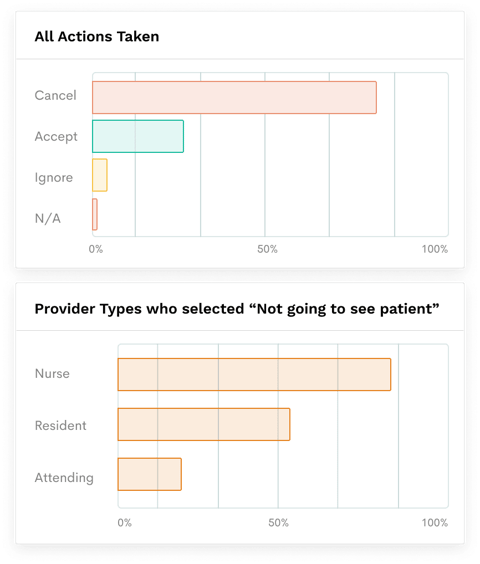
A Phrase Health partner (pediatric academic center) implemented an interruptive alert that advised health care providers to wear an N95 mask when interacting with possible COVID-19 patients that have an order for an aerosol generating procedure. Since the alert fired when providers opened a patient chart, it had a high alert burden (peaking at about 44,000 firings per month).
APPROACH
The client’s informatics team initially justified this because of the alert’s high acceptance rate (~45%). By leveraging Phrase Health’s alert analytics, the team identified providers types that did not need to see the alert by looking at groups frequently selecting the “Not going to see the patient” response.
OUTCOMES
The informatics team fine-tuned the alert triggers to exclude the irrelevant groups andreduced the alert burden by 50%. Additionally, although the team didn’t decide to directly study the effects, they believe the change was also beneficial to a related supply chain initiative to decrease unnecessary usage of N95 masks.
Advanced COVID-19 EHR Alerting
There was minimal knowledge and data exchange in the beginning of the pandemic between providers, labs, and patients. This made it difficult for HonorHealth’s CMIO Dr. Craig Norquist and his team to establish technology to support patient-centered workflows.
APPROACH
To address this, Dr. Norquist and his team created a series of EHR alerts to provide actionable information to clinicians in several ways. One notable achievement was in partnership with HonorHealth’s Health Information Exchange (HIE). At the outset of the pandemic, HonorHealth established the receipt of COVID-19 PCR test results triggered off of HL7 ADT messages (a widely used messaging standard based on movement through a patient journey).
OUTCOMES
Messages from their HIE would trigger alerts and recommend PPE or isolation as soon as a COVID-positive patient arrived at check-in. Per Dr. Norquist, "having lab results from neighboring hospitals or health systems was incredibly helpful in protecting our staff and cutting down on the need for redundant testing at a time when testing supplies were scarce."
Check out more content
Next: Beginner’s Guide to Healthcare Quality Improvement
Previous: “Build versus Buy” for Clinical Process Improvement Technology